Genetic testing for cancer should be the norm now, experts say. Here's when to request it.
Testing is recommended for those with personal and family histories of several types of cancer - including pancreatic and breast cancer
Article Link: https://www.sandiegouniontribune.com/2025/02/25/genetic-testing-for-cancer-should-be-the-norm-now-experts-say-heres-when-to-request-it/
By Netana Markovitz
For The Washington Post
Even though a large proportion of cancer patients carry genetic mutations that make them more susceptible to cancer, only a small percentage of them — and their family members — undergo potentially lifesaving genetic testing, doctors and genetic counselors say.
Genetic testing is recommended for those with personal and family histories of several types of cancer as well as for certain patterns in a family history. The testing is not invasive, and many insurance carriers will cover the cost for cancer patients, yet relatively few people take advantage of what can be a powerful prevention and treatment tool for themselves and their relatives.
“Genetic testing is now absolutely essential to cancer treatment and prevention,” said Allison Kurian, a professor at Stanford Medicine and director of the Stanford Women’s Clinical Cancer Genetics Program. “It’s underused, and I think it’s important for people to talk with their doctors and to talk with their families” about it, Kurian added.
The National Cancer Institute reported in 2023 that “only a small percentage of people diagnosed with cancer undergo” what is known as germline testing, which seeks out gene changes passed along from parents to children. In a study involving nearly 1.4 million people who were diagnosed with cancer from 2013 to 2019, only 6.8 percent underwent germ line testing, researchers wrote in JAMA.
A combination of factors probably reduces testing uptake, including disparities in access, lack of physician recommendations for it and limited genetic counseling resources, experts said.
Who should get tested?
The best person to test first, if feasible, is the family member with cancer.
“The idea has been to find a mutation, to the person who has the condition that is caused by it,” Kurian said. If a mutation is found, then relatives can be tested, in a process called cascade testing.
While many people with genetic mutations may never get cancer, these mutations, if found, confer a higher risk of disease. The implications depend on the specific mutation found.
For example, BRCA gene carriers have a significantly higher risk of several cancers, such as breast, ovarian, pancreatic and prostate cancers. In addition to added screening tests, doctors may suggest considering risk-reducing surgeries and medications. For patients with the BRCA gene who already have cancer, it may influence the type of therapy they receive.
Should I get tested?
People with strong family histories of cancer should feel empowered to seek out testing, regardless of whether a family member with cancer has already been tested, experts said. As a rule of thumb, the closer the relation in the family, the greater the chance you might share a genetic risk. The field is also changing quickly, which means new risk genes are being discovered.
“At this time, mainstream medical guidelines still focus on people who are most likely to have a genetic risk for cancer, which is usually people who have cancer themselves or have a strong family history of cancer, with cancer in multiple relatives and cancer at young ages,” Julie Mak, a genetic counselor and supervisor of the Hereditary Cancer Clinic at the University of California at San Francisco, said via email.
According to Mak, this list is expanding. “The guidelines keep including more people, and some experts in the field have advocated for everyone to be offered this type of testing. … There is a growing argument that cancer genetic testing should be available to more people, maybe everyone who wants it. Right now, there’s still a gap between who we think could benefit from testing and what insurance will cover,” Mak added.
“One of the red flags is a very early age at cancer diagnosis, or multiple cancers in the same person, then interestingly certain kinds of cancers also cluster together in an individual or in families,” said Zsofia Stadler, clinical director of the Clinical Genetics Service and associate attending physician in the Department of Medicine at Memorial Sloan Kettering.
“The same goes for family history, so if there’s a strong family history of early-onset cancers, multiple cancers of the same type or the clustering of certain types [of cancer], those are some of the red flags that we use to demarcate that somebody may be at a higher risk of having an inherited genetic risk for cancer,” she added.
Kurian said people should ask themselves, “Is there cancer in my family? If so, can my relative who had the cancer tell me anything about whether they might have gotten tested? And if not, can my doctor make any recommendations, and where can I find a genetic counselor?”
Why should you get tested?
It’s important to know whether you might carry genetic mutations because it can affect cancer screening recommendations and advice on certain surgical prevention strategies, Kurian said.
“The recommendations from a positive genetic test depend very much on the exact result – which gene and which ‘variant’ or form of the gene — someone has. It’s important to know that some of these results can really significantly change what we recommend in terms of cancer detection and prevention. Others might result in just a small ‘tweak’ to monitoring plans,” Mak wrote.
While medical guidelines frequently change, some of the cancers more commonly associated with risk genes are pancreatic, ovarian, breast, uterine, colon and prostate cancers, according to Stadler, who added that this list is not comprehensive.
The National Comprehensive Cancer Network recommends that all patients with pancreatic adenocarcinoma get genetic testing.
When in doubt, talk with your doctor about your personal and family history of cancer, Kurian said.
Like most medical procedures, there are risks to testing. “For those lower-risk people, we also want to think through the potential costs — not just financial, but also emotional or medical, if they get sent down a road of a lot of extra medical procedures for something kind of minor on their genetic testing,” Mak wrote.
How does testing work?
Generally, testing is ordered by a licensed genetic counselor, but in some cases, it may be ordered by a medical or surgical oncologist.
Testing frequently involves submitting a saliva sample, a cheek swab or a sample of blood. The DNA in the samples is then sequenced by a lab that looks for up to more than 100 gene mutations.
Either an oncologist or a primary care physician may be the one to bring up genetic testing options. But if a physician does not raise the issue, patients should feel empowered to ask whether it’s indicated or for a referral to a genetic counselor, Mak said.
The National Society of Genetic Counselors website also offers guidance on finding genetic counselors.
Is it covered by insurance?
Insurance usually covers genetic testing when it’s guideline-based, but there may be variability and caveats. “Most of the commercial insurances do cover genetic testing if clinical guidelines are met,” Stadler said.
“For people who fall outside of current guidelines, we may run into issues with insurance coverage. That doesn’t mean we can’t do it, but we should be aware that we’re in a transition time where there’s some data to support testing all cancer patients, but the real-life logistics don’t make that easy to implement,” Mak wrote.
Featured News & Stories
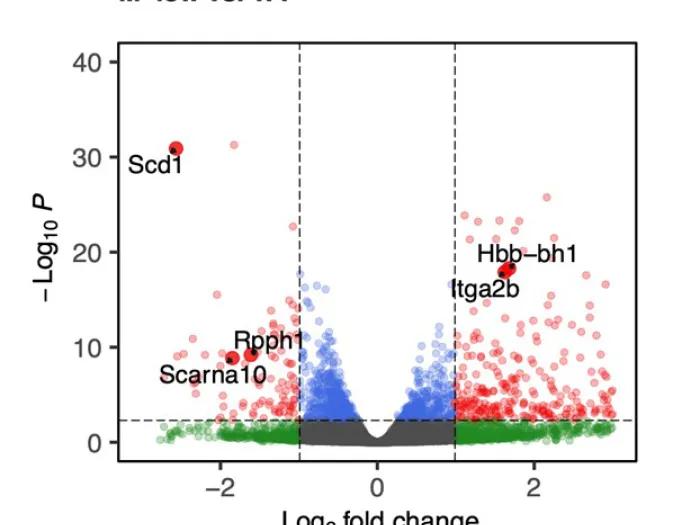
CPOD Faculty Publication Spotlight - Singh Lab

Lung transplant recipient stays active climbing stadium steps and more post-transplant

Medicare's New GLP-1 Bridge Program

University of Michigan Professional Nurse Council reaches tentative agreement with University of Michigan Health
Finding Joy in Leadership: Brian Zink, MD, on Coaching, Purpose and the Next Phase of Academic Medicine
