An Elegant Dance
The role of nerves in oral cancers, from cancer biology to clinical practice
Author |

When tumors present with pain, it is a sign that cancer cells might be in the nerve. In oral squamous cell carcinoma, or OSCC, this feature has been associated with poor prognosis, increased likelihood of disease spread and decreased survival. A growing field of research—cancer neuroscience—aims to understand how cancers and the therapies used to treat them influence the nervous system and vice versa. Discoveries show that the crosstalk between cancer cells and nerves is dynamic and complex.
Nerves play a vital role in the development and functional control of tissue and organs. As discoveries about cancer and nerves began to build, clues have emerged about their interactions, both systemically and within the local tumor microenvironment.
We sat down with Nisha D'Silva, BDS, MSD, Ph.D., an oral and maxillofacial pathologist, cancer biologist, Rogel Cancer Center Scholar and professor at the U-M School of Dentistry, to discuss the communication between cancer and nerves and how knowledge of the mechanisms of how tumors function can improve lives.
Q: Can you describe cancer neuroscience and how the field has evolved in your area of head and neck cancer research?
A: Cancer neuroscience is the multidisciplinary study of cancer-nerve interactions, with the goal of understanding the key players that drive the interaction, and ultimately to use the information to develop specific treatment that disrupts the interaction with the least amount of side effects.
Across cancer types, we know that the nervous system plays an important role in how cancer develops and how it progresses. We have also learned that cancers co-opt the nervous system to amplify cancer growth. Finally, we know that aggressive radiation, which is often used to treat cancer that has invaded nerves, can have long-term debilitating and even harmful effects on patients. But we have no other specific treatment.
Somehow, cancer cells and nerves are attracted to each other. Research has found perineural invasion—or PNI—to be a significant prognostic tool to predict the progression of many cancers, particularly oral cancer, which is my field of expertise. In instances where patients have PNI, they can experience debilitating pain, increased likelihood of cancer spread, and decreased survival. So, if PNI is discovered in the cancer, patients get more aggressive treatment.
As we understand the biology of how cancer and nerves interact, we have to translate this into better diagnosis of PNI, which is what we are doing at present. Also, studying PNI opened other windows into the mechanistic basis of cancer-nerve interactions, leading to the emergence of other neural features, giving further insight on how oral cancers progress, as well as revealing gaps in knowledge to explore in future research.
Q: Can you describe why head and neck cancers are so difficult to treat?
A: Head and neck/oral cancers are challenging to treat due to their proximity to vital anatomical structures in the body that make it possible for human beings to function and survive. There is an increasing incidence of some head and neck cancers in Western countries, which have a high risk of recurrence and are some of the most expensive to treat. Aggressive treatments can lead to decreased quality of life, so the ability to single out which patients are at high risk for recurrence or spread to spare others from difficult and life-altering side effects such as damage to salivary glands, loss of taste, swallowing problems, loss of teeth and more is imperative.
Q: Can you elaborate on how gaps in knowledge have fueled discovery?
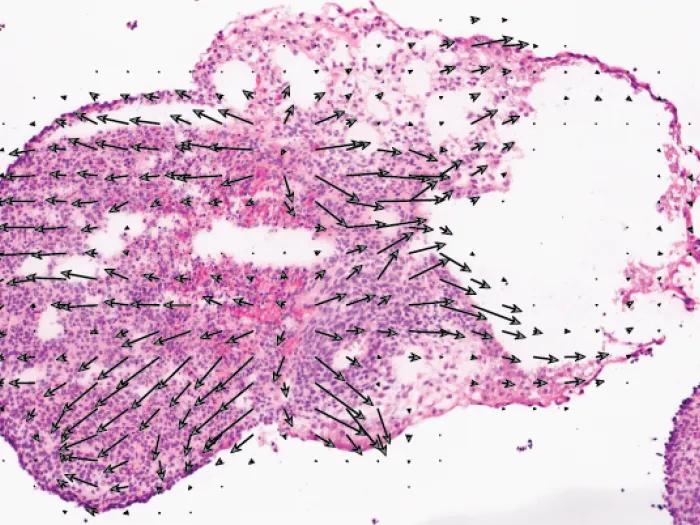
A: One such “a-ha” moment was after our first study on cancer-nerve interactions. We had just completed an intense study teasing apart this elegant dance between cancer and nerves and how they were drawn to each other even before they were in physical contact. While reflecting on these findings and what they meant for a patient, we realized that the findings could change how we currently diagnose PNI and, consequently, could impact treatment selection for patients.
This led to a translational study with clinical specimens and expertise from collaborators at Rogel, Michigan Medicine and the Center for Cancer Biostatistics at the U-M School of Public Health. This study showed that we need to expand our criteria for diagnosing PNI, and that the shorter the distance between a nerve and the nearest tumor island, the poorer the survival. This does not require the cancer to be wrapping around or within the nerves, which is our current definition of PNI. Subsequently, we did a validation study that supported these findings.
Q: How has your research shifted to include other neural phenotypes—beyond PNI—that might be relevant to understanding how OSCC progresses?
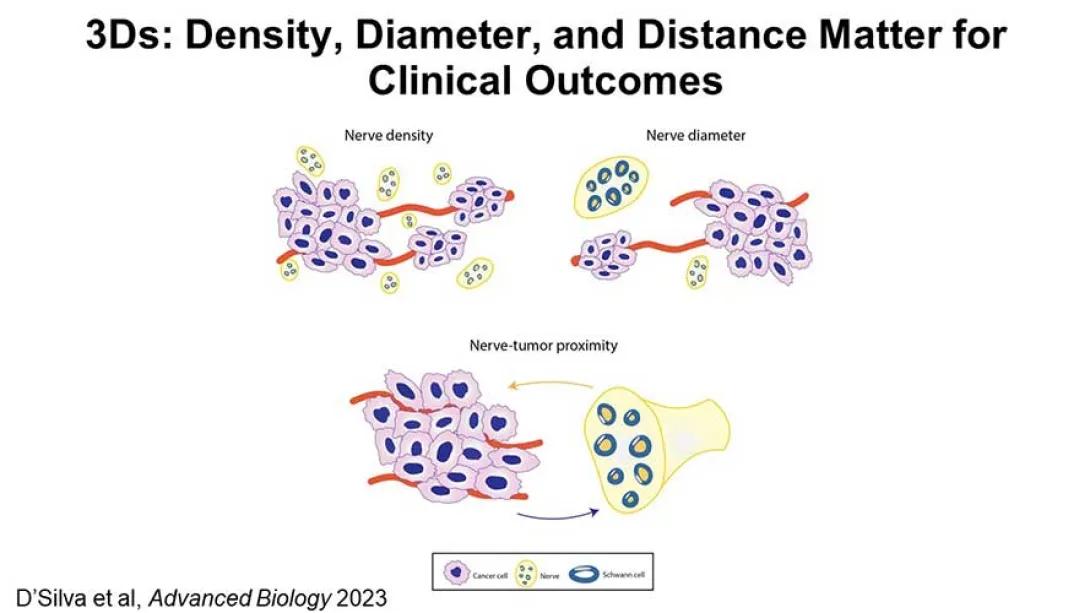
A: Previously the clinical focus of neural features has been entirely on PNI. However, PNI is rarely detectable until the entire tumor is examined. This is a challenge for planning treatment after the initial biopsy. Based on our studies, we suggest that we broaden the neural parameters we assess clinically to include nerve-tumor distance, nerve density and nerve diameter.
A high density of nerves in the tumor enhances tumor progression. However, there are two challenging issues in translating this into clinical practice. First, variation in how nerve density is assessed; and second, nerve density varies by location—the tongue has more nerves than the gums. We found a way to standardize quantification of nerve density and adjust it by site of tumor. Then, we showed that increased nerve density is associated with poor survival.
While large nerve diameter showing PNI is associated with poor survival, large nerves with PNI are so rare in pre-treatment biopsies of oral cancer that they may not be relevant for treatment planning. However, if we consider the diameter of all nerves—not just those with PNI—our data suggest a smaller cut-off. Another way to think of this is that the more nerves with a minimum diameter in the tumor, the greater the possibility of attraction between cancer cells and nerves.
We really need to use a comprehensive set of parameters to decide upon treatment for patients and predict outcomes. We suggest 3Ds: nerve-tumor distance, diameter and density, since they are not mutually exclusive in their effect. Inability to identify one will be compensated by the presence of a different parameter.
We are now teaming up with an international group of pathologists to investigate if we have enough data to support redefining PNI in clinical practice and assessing other neural parameters that may be of clinical relevance. We are also partnering with colleagues in Radiation Oncology to understand the impact of nerve-tumor distance, nerve diameter and nerve density in oral cancer.
Q: How might these new learnings ultimately translate to clinical care?
A: The overall goal is to develop a more personalized approach to select the most appropriate treatment for each individual’s oral cancer so we can improve their survival and their quality of life after treatment. Our goal is to translate significant findings from our complex studies on the biology of cancer-nerve interactions to universal criteria that would be cost-effective and easily deployable in variably resourced clinical settings.
Q: How is the Rogel Cancer Center working to bring together collective knowledge of clinicians and scientists working in cancer neuroscience?
A: Something that I find really exciting about the University of Michigan and the Rogel Cancer Center is the cross-disciplinary collaboration in research and care. It has been amazing to team up with clinicians and scientists with different expertise to develop resources and identify markers that can then be used to enhance clinical care.
An important new initiative is the Cancer Neuroscience working group to galvanize interactions between cancer biologists and neuroscientists on campus to investigate communication between cancer and nerves during tumor progression. I met Muneesh Tewari, M.D., Ph.D., a medical oncologist, fortuitously on a plane when we were both headed for the same cancer neuroscience meeting and decided to develop some synergy in this area. We were strongly encouraged by Eric Fearon, M.D., Ph.D., the director of the Rogel Cancer Center, who provided resources to start a working group. We have been meeting in smaller groups and had our first working group retreat last summer. These interactions have already resulted in multiple grant applications and a publication.
I believe the culture at the Rogel Cancer Center values the importance of basic science discoveries and translating them into clinical care. Our group has played a role in identifying important features of nerves in oral cancer that could predict response to treatment, as well as finding new targets to interrupt the interactions between nerves and cancer, both with the ultimate goal of benefiting patients who are diagnosed with this aggressive cancer.
Further reading on this topic:
- The D'Silva Lab
- D'Silva NJ, Perez-Pacheco C, Schmitd LB. The 3D's of Neural Phenotypes in Oral Cancer: Distance, Diameter, and Density. Adv Biol (Weinh). 2023 Feb;7(2):e2200188. doi: 10.1002/adbi.202200188. Epub 2022 Nov 14. PMID: 36373694; PMCID: PMC9957924.
Keep Reading Illuminate 2026:
- The Answers in the Epigenome
- Emerging into the Future
- Closing the Gap
- The Next Generation 2026
- Helping Patients Make Longer-Term Treatment Choices During Survivorship
Learn more:

Illuminate
Articles showcasing the latest in cancer research underway at the Rogel Cancer Center
Featured News & Stories

MYHealth team publishes findings about positive effects of MYHealth youth research program

2026 Global Health Annual Update

Many young adults may not be ready to manage their own health care
CPOD Faculty Publication Spotlight - Welch Lab

What should you know before starting a GLP-1?
