MAPLE/POPLAR/BIRCH

Research Overview
The MAPLE study focuses on the impacts of federal and state behavioral health policy changes on health and economic outcomes during pregnancy and after birth. The supplemental POPLAR study focuses specifically on maternal morbidity and mortality, while the supplemental BIRCH study focuses on delivering mothers with substance use disorders and their infants.
Publications
Birth outcomes among people with treated and untreated perinatal mood and anxiety disorder during pregnancy
Perinatal mood and anxiety disorders (PMAD) represent common and burdensome comorbidities of pregnancy and postpartum. They increase risk of adverse maternal birth outcomes including cesarean birth and severe maternal morbidity (SMM). Whether antenatal mental health treatment can improve these birth outcomes among people with PMAD remains unknown. Dr. Stephanie V. Hall led this cross-sectional analysis of commercial insurance claims to determine if people with treated PMAD during pregnancy experience lower rates of adverse birth outcomes than those with untreated PMAD during pregnancy.
Findings: This study found people with PMAD and documented mental health treatment during pregnancy experienced similar odds of primary cesarean birth and SMM as those with no documented mental health treatment.
Meaning: Prior studies found psychotropic drugs are associated with decreased cesarean birth when comparing those with treated PMAD to those without PMAD. This study indicates this difference may be attributable to differences in PMAD status rather than treatment.
Evaluating maternal-infant healthcare utilization and costs among individuals experiencing perinatal mood and anxiety disorders
Maternal-infant outcomes are often reported separately, yet the maternal-infant connection is fundamental for the psychological wellbeing of both individuals and their overall health. Dr. Ashlee J. Vance let this study evaluating parallel healthcare utilization outcomes and costs for maternal-infant dyads during the postpartum period for those with and without perinatal mood and anxiety disorders (PMAD).
Findings: The sample consisted of 101,306 birthing individuals and 108,438 infants representing 108,438 unique dyads. Individuals with pre- or post-delivery PMAD had higher rates of NICU admissions (13.6% and 11.4%, respectively) than those without PMAD (9.9%). Emergency department visits and outpatient utilization decreased over time for both birthing individuals and infants overall. Odds of outpatient services utilization were highest among deliveries with post-PMAD present (newborn outpatient services aOR: 1.687, CI: 1.274, 2.233 and birthing individual outpatient services aOR: 6.48, CI: 5.490, 7.648). The PMAD+substance use disorder (PMAD+SUD) group had the highest dyadic out-of-pocket costs (median: $798.32, IQR: $316.20, $1,943.74), and the post-delivery PMAD group had the second highest dyadic costs (median: $505.95, IQR: $211.29, $1,169.01), a difference of almost $300.
Meaning: Results from this study demonstrate significant differences among PMAD groups (i.e., pre-delivery, post-delivery, co-occurring PMAD and SUD) compared to a group without PMAD. This might suggest that PMAD status influences changes in healthcare use or costs. Additionally, the percentage of both birthing people and their infants using outpatient services remained nearly identical during the study period, further emphasizing the connection between the dyad and healthcare use.
View Maternal Health, Neonatology and Perinatology Article
We Need Maternal Mental Health Data Systems That Leverage Existing Data And Platforms
In this article for Health Affairs Forefront article, the study team discussed how, in order to identify needs and provide adequate care for perinatal women with mental health conditions, we must learn more about the pervasiveness and extent of untreated mental health conditions.
Excerpt: “We know that the maternal health crisis is complicated by our significant lack of data and slow translation of research evidence to improved policy and practice. The US lags behind the rest of the world by not having access to high-quality maternal mental health data, as evidenced by lack of a national depression or anxiety prevalence rate that includes both privately and publicly insured people during pregnancy or in the year after birth, known as the perinatal period. The best estimate is that one in five people experience a mental health problem during pregnancy or in the perinatal period. When untreated, maternal mental health problems represent a major risk for infants, mothers, and the entire family—for example, infant health problems at birth and maternal suicidality in the year after giving birth. Unfortunately, most perinatal women do not get the mental health treatment that they need. Therefore, maternal mental health in the US remains unaddressed as the most pressing national priority to improve health outcomes for perinatal women and infants.”
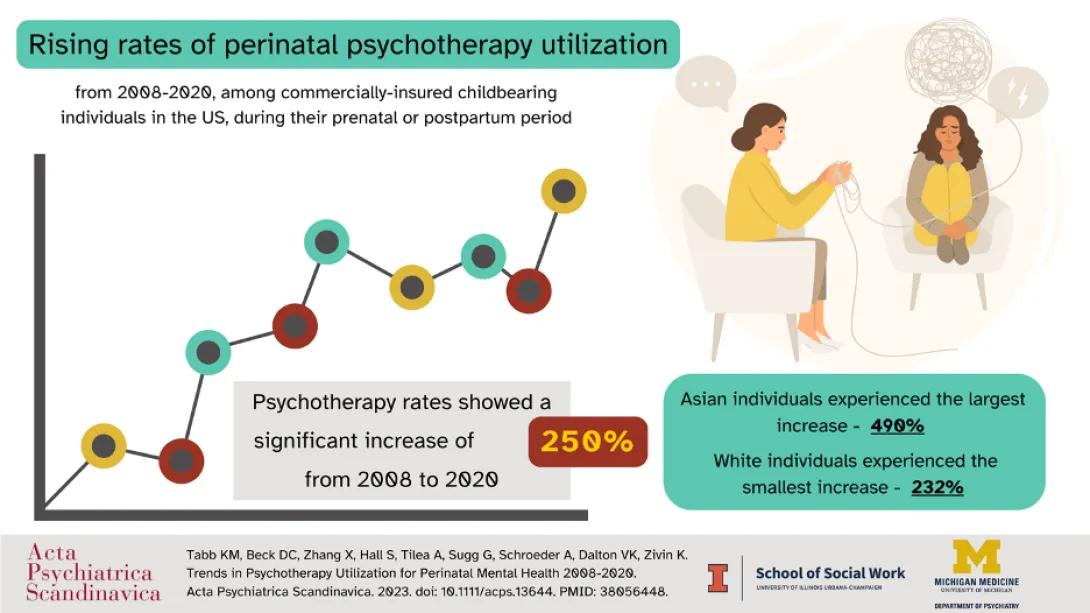
Visual abstract depicting key study findings. In this study titled "Trends in Psychotherapy Utilization for Perinatal Mental Health 2008-2020," psychotherapy rates showed a significant increase of 250% among commercially insured U.S. individuals during their perinatal or postpartum period. Asian individuals experienced the largest increase of 490%, and white individuals experienced the smallest increase of 232%.
Trends in psychotherapy utilization for perinatal mental health 2008-2020
Dr. Karen M. Tabb led this study aiming to characterize trends in psychotherapy utilization during the prenatal or postpartum period among commercially insured individuals aged 15–44.
Findings: Psychotherapy rates showed a significant increase of 250%, from 1,091 (95% CI: 1067–1115) per 10,000 individuals in 2008 to 2,726 (95% CI: 2,687–2,764) per 10,000 individuals in 2020. White individuals recorded the highest rates, followed by Black, Hispanic, and Asian groups, respectively. The most significant increase in crude psychotherapy rates was observed among Asian individuals, with a 490% surge from 423 (95% CI: 363–484) per 10,000 individuals in 2008 to 2,073 (95% CI: 1936 – 2209) per 10,000 individuals in 2020. In contrast, psychotherapy rates among White individuals demonstrated the least growth compared to other racial groups, with a 232% increase from 1,255 (95% CI: 1,222–1,288) per 10,000 in 2008 to 2,909 (95% CI: 2,859–2,959) per 10,000 in 2020.
Meaning: Perinatal psychotherapy utilization among commercially insured adults increased upward over a 12-year period; however, clear differences in utilization across racial categories persist. The research findings presented provide evidence for differential rates of mental health service use, which can inform efforts towards mental health equity.
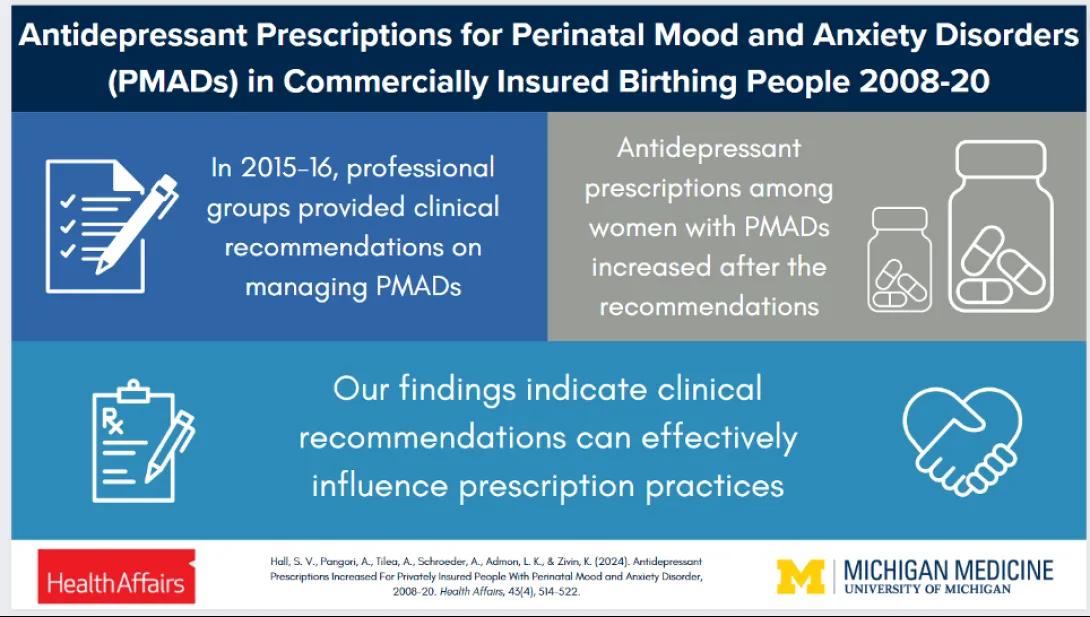
Visual abstract depicting study findings. In this study titled "Antidepressant Prescriptions Increased for Privately Insured People with Perinatal Mood and Anxiety Disorders (PMAD)," we found that antidepressant prescriptions among women with PMADs increased after professional groups provided clinical recommendations on managing PMAD. Our findings indicate that clinical recommendations can effectively influence prescribing practices.
Antidepressant Prescriptions Increased For Privately Insured People With Perinatal Mood and Anxiety Disorder
Dr. Stephanie V. Hall led this work on how clinical recommendations from professional groups impacted antidepressant prescription practices for women with perinatal mood and anxiety disorders (PMAD) for commercially insured people in the US. Health Affairs featured this work both in their publication and as an invited presentation in their April 2024 edition of the Health Affairs briefing agenda panel “Improving Access to Care.”
Findings: For individuals with antenatal PMAD, the odds of an antenatal antidepressant prescription decreased 3 percent annually from 2008-2016 and increased by 32 percent in 2017, and the annual rate of change increased 5% for 2017-2020 compared to 2008-2016. For individuals with postpartum PMAD, the odds of a postpartum antidepressant prescription decreased 2 percent annually from 2008-2016, experienced no significant change in 2017, but the annual rate of change increased 3 percent for 2017-2020 compared to 2008-2016.
Meaning: The clinical recommendations issued in 2015 and 2016 were associated with increased antidepressant prescriptions for PMAD, particularly for antenatal PMAD. These findings indicate clinical recommendations represent an effective tool for changing prescribing patterns.
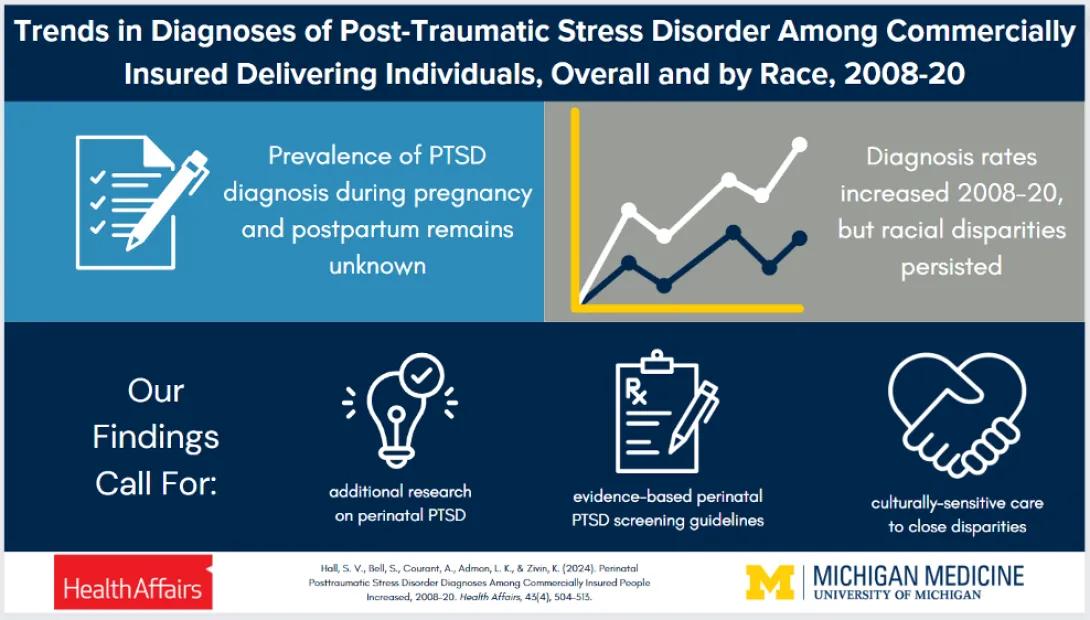
Visual abstract depicting study findings. In this study titled "Trends in Diagnoses of Post-Traumatic Stress Disorder (PTSD) Among Commercially Insured Delivering Individuals, Overall and by Race, 2008-20," we found that while prevalence of PTSD diagnoses during pregnancy and postpartum remains unknown, diagnoses rates increased 2008-20 and racial disparities persisted. Our findings call for additional research on perinatal PTSD, evidence-based perinatal PTSD screening guidelines, and culturally sensitive care to close disparities.
Trends in Diagnoses of Post-Traumatic Stress Disorder Among Commercially Insured Delivering Individuals, Overall and by Race, 2008-20
Dr. Stephanie V. Hall led this work on trends in PTSD diagnoses during the perinatal period for commercially insured delivering individuals, overall and by race. Health Affairs featured this work both in their publication and as an invited presentation in their April 2024 edition of the Health Affairs Journal Club.
Findings: We observed a 394% increase in perinatal PTSD diagnoses from 37.7 per 10,000 deliveries in 2008 to 186.3 per 10,000 deliveries in 2020. White individuals had the highest diagnosis rate at all timepoints (208.0 per 10,000 deliveries in 2020) followed by Black, unknown/missing race, Hispanic, and Asian individuals (188.7, 171.9, 146.9, and 79.8 per 10,000 deliveries in 2020, respectively).
Meaning: The significant growth of perinatal PTSD diagnosis rates may reflect increased awareness, diagnosis, and/or prevalence of the disorder. However, these rates fall well below the estimated prevalence of PTSD in the perinatal population.
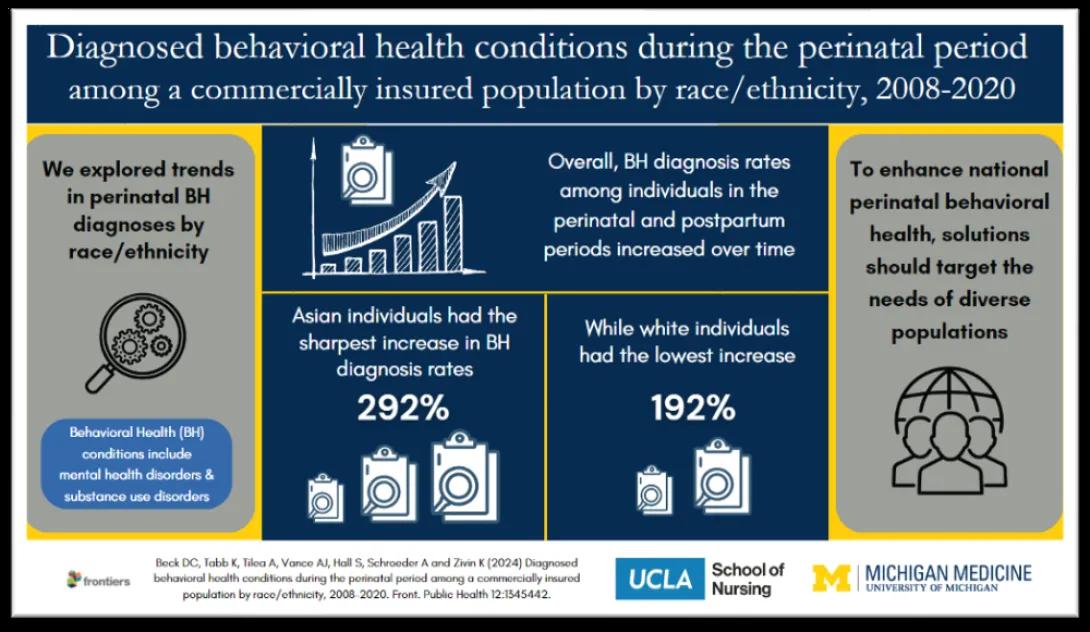
Visual abstract depicting study findings. In this study titled "Diagnosed Behavioral Health Conditions During the Perinatal Period Among a Commercially Insured Population by Race/Ethnicity, 2008-2020," we explored trends in perinatal behavioral health diagnoses by race and ethnicity.
Diagnosed Behavioral Health Conditions During the Perinatal Period Among a Commercially Insured Population by Race/Ethnicity, 2008-2020
Dr. Dana Beck led this project to examine trends in diagnosed behavioral health (BH) conditions [mental health (MH) disorders or substance use disorders (SUD)] among pregnant and postpartum individuals between 2008-2020. We then explored the relationship between BH conditions and race/ethnicity, acknowledging race/ethnicity as a social construct that influences health disparities.
Findings: In adjusted analyses, white individuals experienced the highest rates of BH conditions, followed by Black, Hispanic, and Asian individuals, respectively. Asian individuals had the largest increase in BH rates, increasing 292%. White individuals had the smallest increase of 192%. The trend remained unchanged even after adjusting for age and Bateman comorbidity score, the trend remained unchanged.
Meaning: The prevalence of diagnosed BH conditions among individuals in the perinatal and postpartum periods increased over time. As national efforts continue to work toward improving perinatal BH, solutions must incorporate the needs of diverse populations to avert preventable morbidity and mortality.
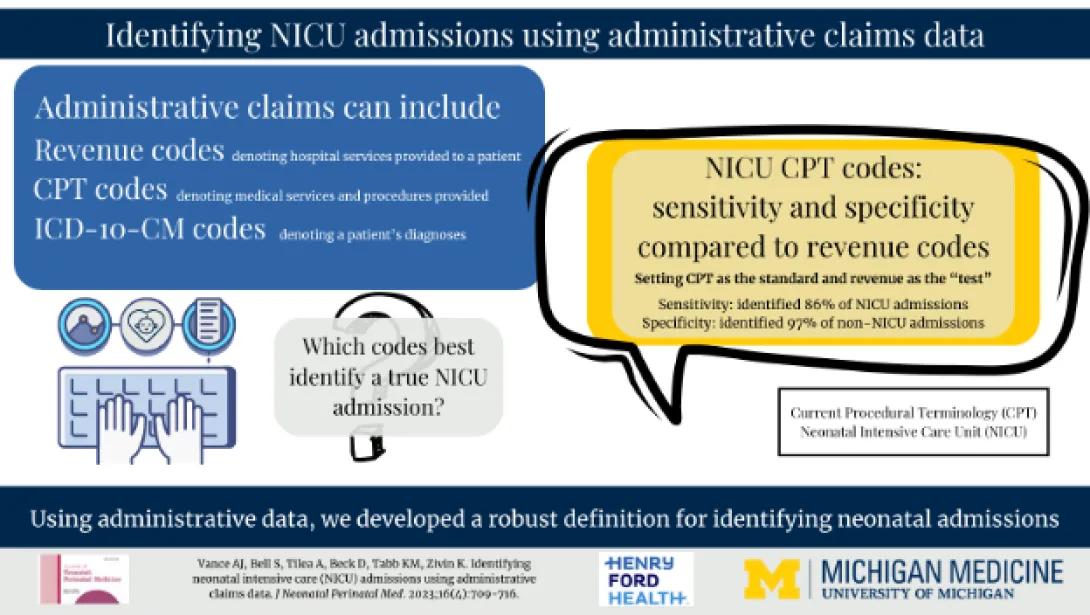
Visual abstract depicting study findings. In this study titled "Identifying neonatal intensive care (NICU) admissions using administrative claims data," we define a method for identifying neonatal intensive care unit (NICU) admissions using administrative claims data.
Identifying neonatal intensive care (NICU) admissions using administrative claims data
Dr. Ashlee J. Vance led this study aimed to define a method for identifying neonatal intensive care unit (NICU) admissions using administrative claims data.
Findings: On average, revenue codes (3.3%) alone identified more NICU hospitalizations compared to Current Procedural Terminology (CPT) codes alone (1.5%), whereas the use of CPT and revenue (8.9%) and CPT or revenue codes (13.7%) captured the most NICU hospitalizations, which aligns with rates of preterm birth. Gestational age alone (4.2%) and birthweight codes alone (2.0%) identified the least number of potential NICU hospitalizations. Setting CPT codes as the standard and revenue codes as the "test," revenue codes resulted in identifying 86% of NICU admissions (sensitivity) and 97% of non-NICU admissions (specificity).
Meaning: Using administrative data, we developed a robust definition for identifying neonatal admissions. The identified definition of NICU codes is easily adaptable, repeatable, and flexible for use in other datasets.
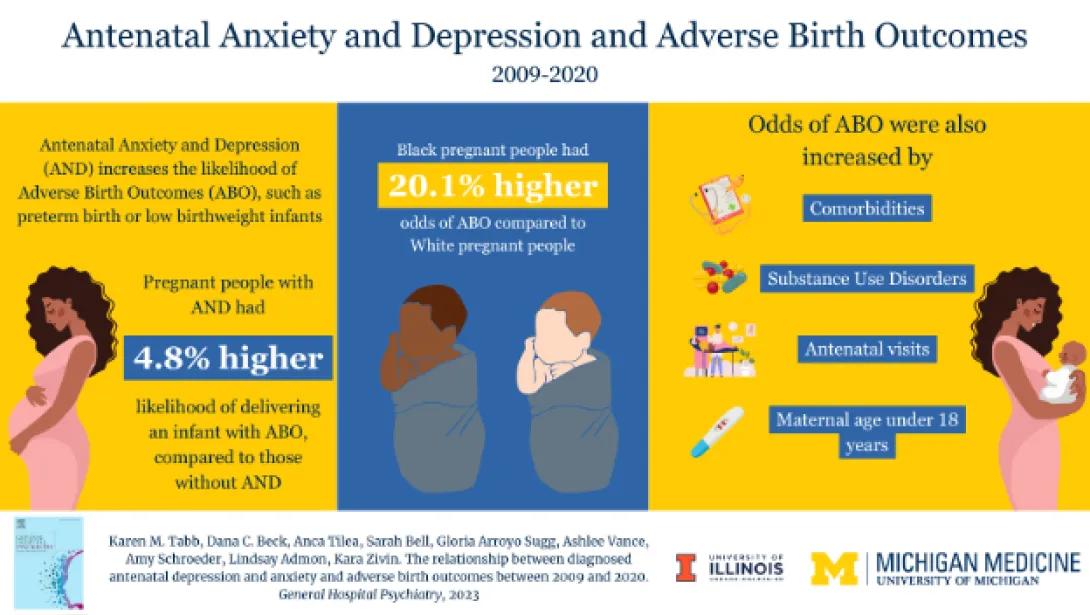
Visual abstract depicting key study findings. This study titled "The Relationship between Diagnosed Antenatal Depression and Anxiety and Adverse Birth Outcomes between 2009 and 2020" found that people with antenatal anxiety or depression (AND) had a 4.8% higher likelihood of delivering an infant with adverse birth outcomes (ABO) compared to perinatal women without AND, as did Black perinatal women compared to White perinatal women (20.1% higher likelihood). Odds were increase by comorbidities, substance use disorders, antenatal visits, and maternal age under 18 years.
The relationship between diagnosed antenatal depression and anxiety and adverse birth outcomes between 2009 and 2020
Dr. Karen M. Tabb led this retrospective cohort study examined trends in adverse birth outcomes (ABO) among perinatal commercially insured women aged 15–44.
Findings: This study found perinatal women with antenatal anxiety or depression (AND) had a higher likelihood of delivering an infant with ABO compared to perinatal women without AND, as did Black perinatal women compared to White perinatal women.
Meaning: Interventions to address the mental health of Black perinatal women, such as respectful care or peer navigation, are needed to potentially improve infant outcomes.
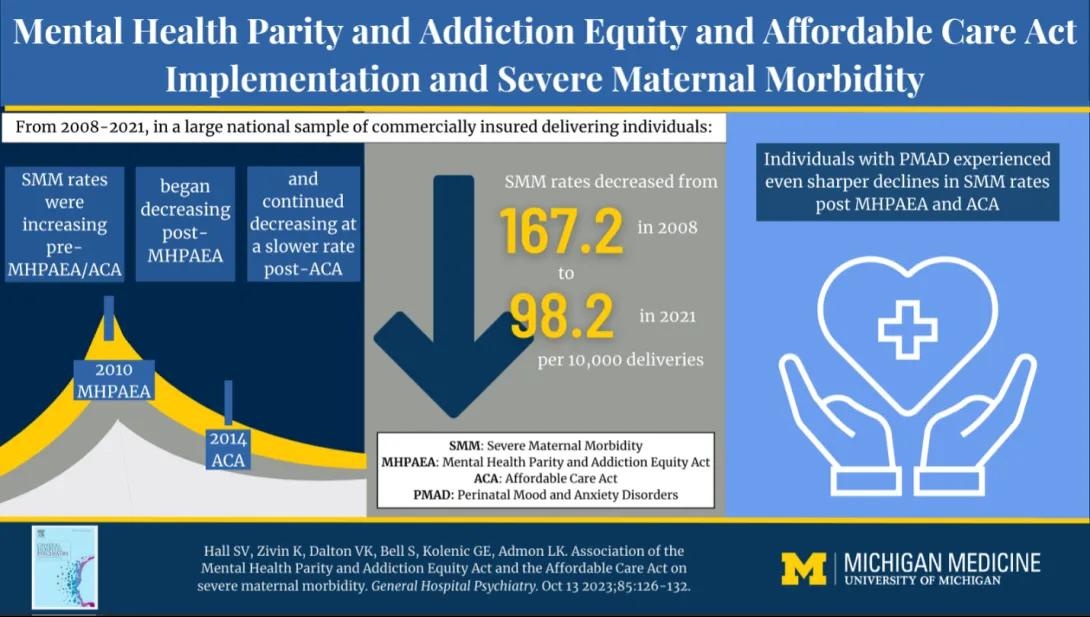
Visual abstract depicting study findings. In this study titled "Association of the Mental Health Parity and Addiction Equity Act (MHPAEA) and the Affordable Care Act (ACA) on severe maternal morbidity (SMM)," from 2008-2021 in a large national sample of commercially insured individuals, SMM rates were increasing pre-MHPAEA/ACA, began decreasing post-MHPAEA, and continued decreasing at a slower rate post-ACA. Adjusted SMM rates declined from 167.2 in 2008 to 98.2 in 2021 per 10,000 deliveries in the last quarter of 2021. Individuals with perinatal mood and anxiety disorders experienced even sharper declines in SMM post-MHPAEA/ACA.
Association of the Mental Health Parity and Addiction Equity Act and the Affordable Care Act on severe maternal morbidity
Dr. Stephanie V. Hall led this research to characterize the association between Mental Health Parity and the Affordable Care Act and rates of severe maternal morbidity among a population of commercially insured individuals, including individuals with and without perinatal mood and anxiety disorders.
Findings: Adjusted severe maternal morbidity rates declined from 167.2 (95%CI: [152.6, 181.9]) per 10,000 deliveries in the first quarter of 2008 to 98.2 (95%CI: [83.5, 112.8]) per 10,000 deliveries in the last quarter of 2021.
Meaning: The observed association suggests implementation of Mental Health Parity and Affordable Care Act may have played a role in lowering rates of severe maternal morbidity, particularly among individuals with perinatal mood and anxiety disorders.
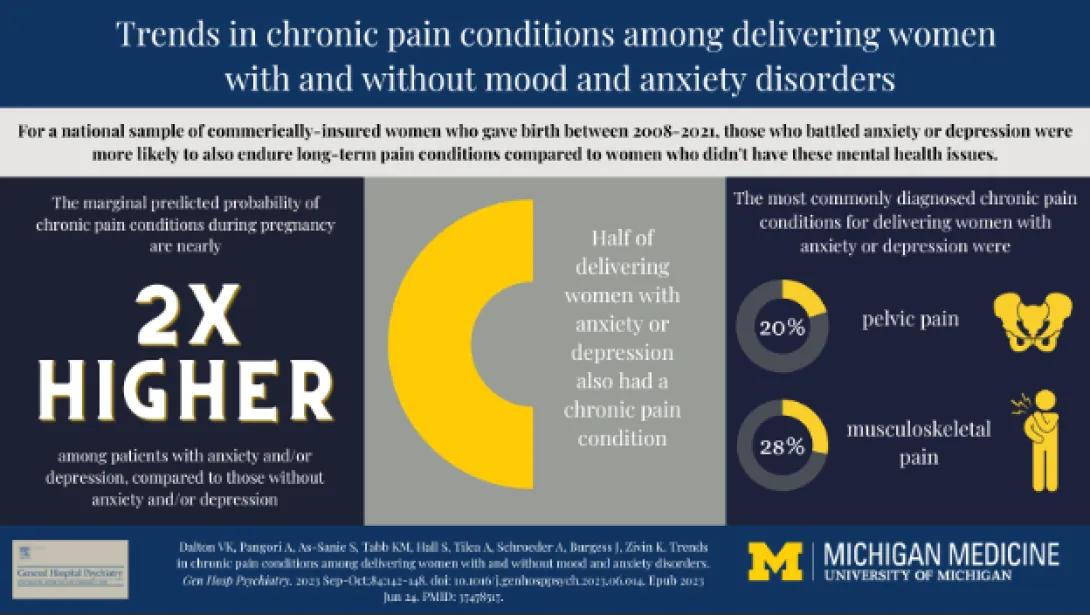
Visual abstract depicting key study findings. In this study titled "Trends in Chronic Pain Conditions among Delivering Women with and without Mood and Anxiety Disorders," in a national sample of commercially insured women who gave birth between 2008 and 2021, those with anxiety and depression were more likely to experience long-term pain conditions compared to those without mental health conditions. The marginal predicted probability of chronic pain conditions during pregnancy is twice higher among patients with anxiety and/or depression compared to those without these conditions. Half of delivering women with anxiety and/or depression also had a chronic pain condition, most commonly pelvic pain (20%) and musculoskeletal pain (28%).
Trends in chronic pain conditions among delivering women with and without mood and anxiety disorders
Dr. Vanessa K. Dalton led this study, which sought to describe trends in chronic pain among a sample of delivering women and describe the coexistence of chronic pain with anxiety and/or depression among delivering women.
Findings: Musculoskeletal and pelvic pain occurred most often regardless of delivering status. Delivering women with anxiety and/or depression had higher marginal predicted probabilities of chronic pain compared to all delivering women. Between 2008 and 2021, the predicted probabilities ranged from 0.400 to 0.527 and 0.221-0.261, respectively.
Meaning: The frequency of comorbid depression and/or anxiety with pain disorders among delivering women highlights the importance of proper detection, coordination of care, and safe treatment options for this population.
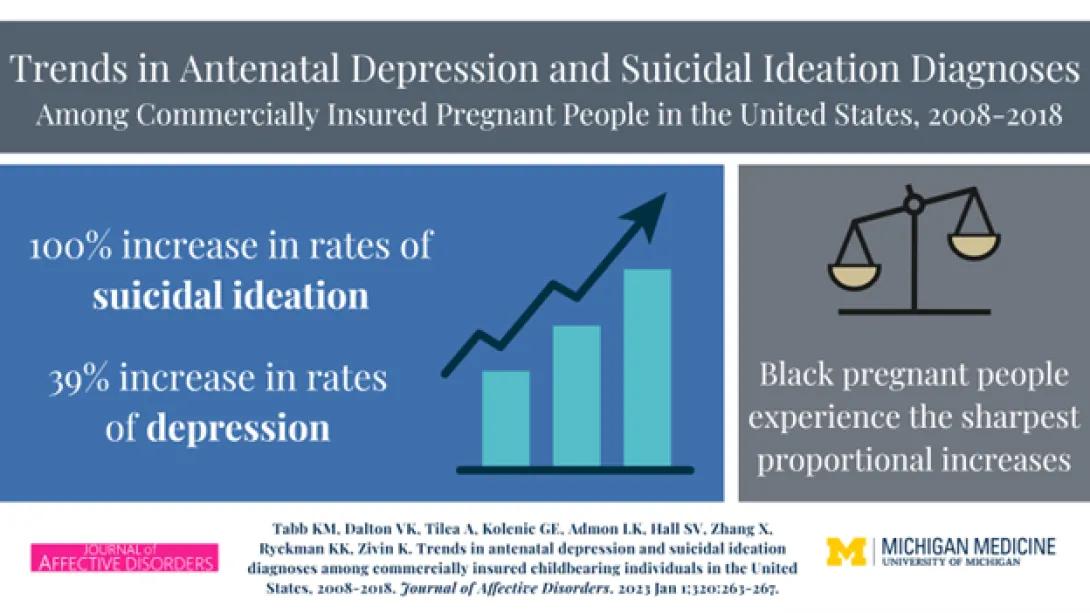
Visual abstract depicting key study findings. In this study titled "Trends in Antenatal Depression and Suicidal Ideation Diagnoses among Commercially Insured Childbearing Individuals in the United States, 2008-2018," rates of depression increased by 39% and suicidal ideation increased by 100% in 2018. Black women experienced the sharpest proportional increases.
Trends in antenatal depression and suicidal ideation diagnoses among commercially insured childbearing individuals in the United States, 2008-2018
Dr. Karen Tabb with the University of Illinois Urbana-Champaign led a paper with our group on antenatal depression and suicidal ideation diagnoses among U.S. people with commercial insurance policies.
Findings: Rates (95 % CIs) of antenatal depression increased by 39 % from 540 (520-560) per 10,000 individuals in 2008 to 750 (730-770) per 10,000 individuals in 2018. Antenatal suicidal ideation increased by 100 % from 15 (12-18) per 10,000 individuals in 2008 to 44 (39-50) per 10,000 individuals in 2018. Black women experienced the sharpest proportional increases.
Meaning: The prevalence of depression and suicidal ideation occurring during pregnancy substantially increased over a ten-year period. Further, suicidal ideation diagnosis increased the most for among Black women compared to all groups, resulting in a need for future studies in this area to determine the reasons for an increase in diagnosis and any change in resulting treatment of follow up.
View Journal of Affective Disorders Article
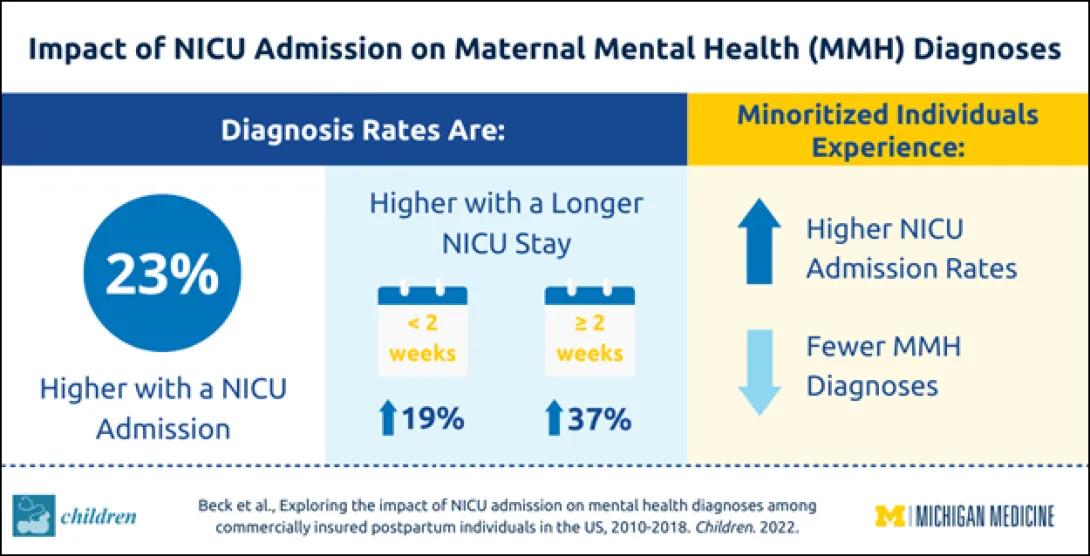
Visual abstract depicting key study findings. In this study titled "The Association between NICU Admission and Mental Health Diagnoses among Commercially Insured Postpartum Women in the US, 2010–2018," mental health (MH) diagnoses were 23% higher with a NICU admission. Women whose infants became hospitalized in the NICU for <2 weeks had 19% higher odds of maternal MH diagnoses and those whose infants became hospitalized for >2 weeks had 37% higher odds of maternal MH diagnoses compared to those whose infants did not have a NICU hospitalization. Minoritized individuals experienced higher NICU admission rates and fewer MH diagnoses
The Association between NICU Admission and Mental Health Diagnoses among Commercially Insured Postpartum Women in the US, 2010–2018
Dr. Dana Beck, now with UCLA, led this work on how a NICU admission and its duration affects maternal mental health (MMH) diagnoses.
Findings: Women whose infants became hospitalized in the NICU for <2 weeks had 19% higher odds of maternal MH diagnoses and those whose infants became hospitalized for >2 weeks had 37% higher odds of maternal MH diagnoses compared to those whose infants did not have a NICU hospitalization. Compared to white women, all other race/ethnicities had significantly lower odds of receiving a maternal MH condition diagnosis despite higher rates of NICU hospitalization.
Meaning: These findings suggest a need to target the NICU to improve maternal MH screening, services, and support while acknowledging the influence of social determinants, including race and ethnicity, on health outcomes.
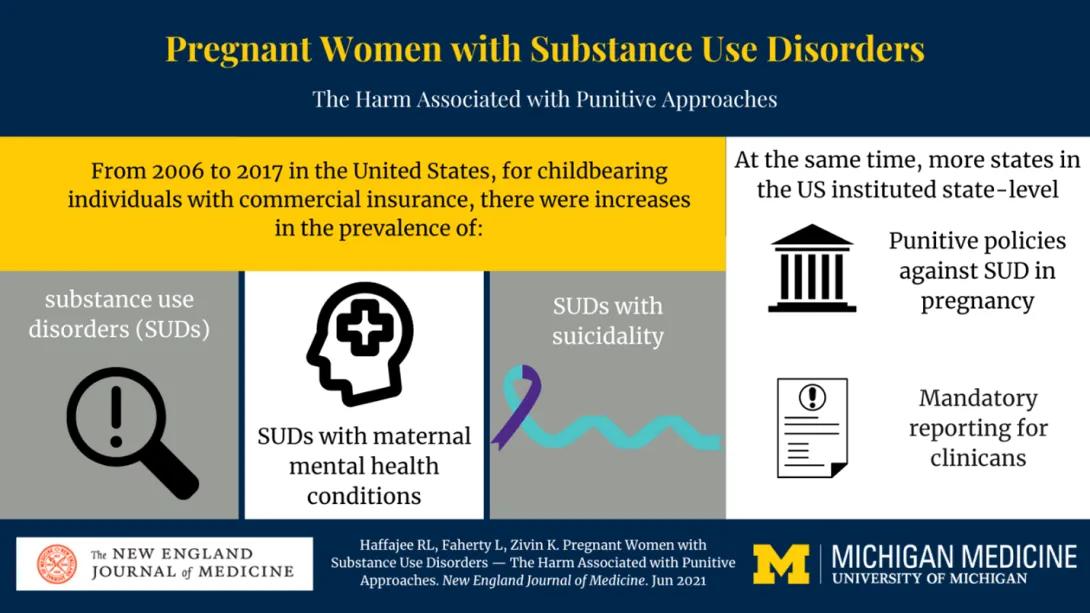
Visual abstract depicting key study findings. In this study titled "Pregnant Women with Substance Use Disorders — The Harm Associated with Punitive Approaches," for pregnant women with commercial insurance in the United States, the prevalence of substance use disorders (SUDs), SUDs cooccurring with maternal mental health conditions, and SUDs cooccurring with suicidality all increased from 2006 to 2017. At the same time, more states in the US instituted state-level punitive policies against SUD in pregnancy and mandatory reporting for clinicians.
Pregnant Women with Substance Use Disorders — The Harm Associated with Punitive Approaches
Drs. Rebecca Haffajee, Laura Faherty, and Kara Zivin published a perspective article in the New England Journal of Medicine on state-level punitive and reporting policies on substance use disorders during pregnancy.
Findings: For childbearing women with commercial insurance in the United States, the prevalence of substance use disorders (SUDs), SUDs cooccurring with maternal mental health conditions, and SUDs cooccurring with suicidality all increased from 2006 to 2017. During the same time, there was a steady increase in the number of States with punitive and reporting policies on the detection of substance use during pregnancy.
Meaning: Amid increasing rates of behavioral health conditions in this population, persistent adverse maternal health outcomes, and the COVID-19 pandemic (during which overdose deaths have spiked), we need policies that draw women into care and help them recover, not policies that push them away from care and into the criminal justice system. Punishing pregnant women with SUDs has been ineffective; we believe it’s time to prioritize approaches that support pregnant women and their families.
View New England Journal of Medicine Article
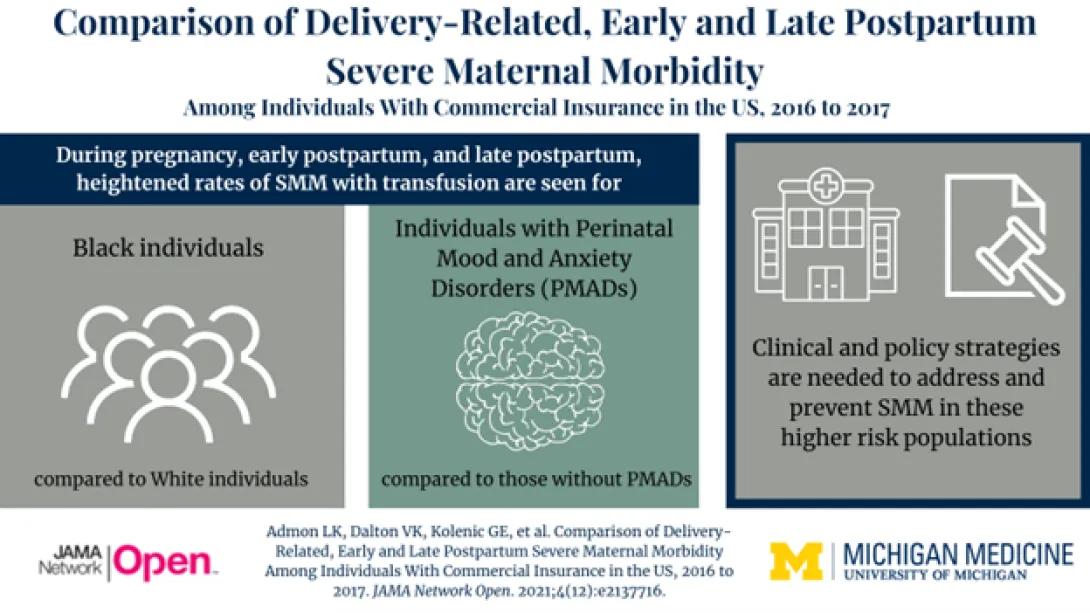
Visual abstract depicting key study findings. In this study titled "Comparison of Delivery-Related, Early and Late Postpartum Severe Maternal Morbidity Among Individuals with Commercial Insurance in the US, 2016 to 2017," higher rates of severe maternal morbidity (SMM) with transfusion occurred among Black individuals compared to White individuals for the pregnancy, early postpartum, and late postpartum periods. We also saw higher rates of SMM with transfusion in individuals with PMADs compared to those without PMADs in each of the three periods. These findings should inform clinical and policy strategies to address and prevent maternal morbidity and mortality among these populations.
Comparison of Delivery-Related, Early and Late Postpartum Severe Maternal Morbidity Among Individuals With Commercial Insurance in the US, 2016 to 2017
Dr. Lindsay Admon published a research letter entitled, “Comparison of Delivery-Related, Early and Late Postpartum Severe Maternal Morbidity Among Individuals with Commercial Insurance in the US, 2016 to 2017.”
Findings: Higher rates of severe maternal morbidity (SMM) with transfusion occurred among Black individuals compared to White individuals for the pregnancy, early postpartum, and late postpartum periods. Higher rates of SMM with transfusion were also seen in individuals with PMADs compared to those without PMADs in each of the three periods.
Meaning: Black individuals and individuals with PMADs experienced a markedly sustained risk for SMM early and late postpartum, which should inform clinical and policy strategies to address and prevent maternal morbidity and mortality among these populations.
Visual abstract depicting key study findings. In this study titled "Trends in Primary Cesarean Section Rates among Women with and without Perinatal Mood and Anxiety Disorders (PMAD)," the predicted probability of a C-section was on average 3.5% higher for women with PMADs than those without them. Annual C-section decreased for both groups during the study period. Primary C-sections occurred at clinically and statistically significant higher rates among otherwise low-risk women with PMAD.
Trends In Primary Cesarean Section Rates Among Women With And Without Perinatal Mood And Anxiety Disorders
Melissa Zochowski led this project on primary Cesarean section trends among women with and without PMADs, in a commercially insured US population from 2007-2018.
Findings: The predicted probability of a C-section was on average 3.5% higher for women with PMADs than those without them (95% CI: 2.7, 4.3). Annual C-section rates fell during the study period for both groups, with rates decreasing from 26.8% in 2008 to 21.8% in 2017 for the PMAD group, and from 23.2% in 2008 to 18.2% in 2017 for the group without PMAD diagnoses.
Meaning: PMADs were associated with higher rates of primary C-section in a population of women otherwise at low risk for delivery by C-section. This finding extends what is known about the relationship between these disorders and a critical birth outcome, implicating that primary C-sections may be an important negative birth income to include in future analyses of women with PMADs who are otherwise at low risk for delivery by C-section.
Visual abstract depicting key study findings. In this serial cross-sectional analysis of individuals 1 year before and after giving birth, suicidal ideation and intentional self-harm increased significantly between 2006 and 2017. Non-Hispanic Black individuals, those with low-income, and younger individuals as well as those with comorbid anxiety, depression, or other serious mental illness had larger escalations.
Trends in Suicidality 1 Year Before and After Birth Among Commercially Insured Individuals in the United States, 2006-2017
Dr. Lindsay Admon led this research to assess the trends in suicidal ideation and intentional self-harm in a large national cohort of commercially insured individuals.
Findings: In this serial cross-sectional analysis of 595 237 individuals 1 year before and after giving birth, suicidal ideation and intentional self-harm increased significantly between 2006 and 2017. Non-Hispanic Black individuals, those with low-income, and younger individuals as well as those with comorbid anxiety, depression, or other serious mental illness had larger escalations.
Meaning: Clinical and policy interventions for addressing this health crisis should be tailored to meet the unique needs of individuals in the year before and following birth, particularly among high-risk groups.